Adenoidid refers to the inflammation or enlargement of the adenoid glands located at the back of the nasal passage, just above the throat. Furthermore, this condition affects breathing, sleep quality, hearing, and overall immune function in ways that significantly disrupt daily life. This comprehensive guide covers everything patients and caregivers need to understand about recognizing, diagnosing, and treating this condition effectively.
What Are Adenoids and Why Do They Matter
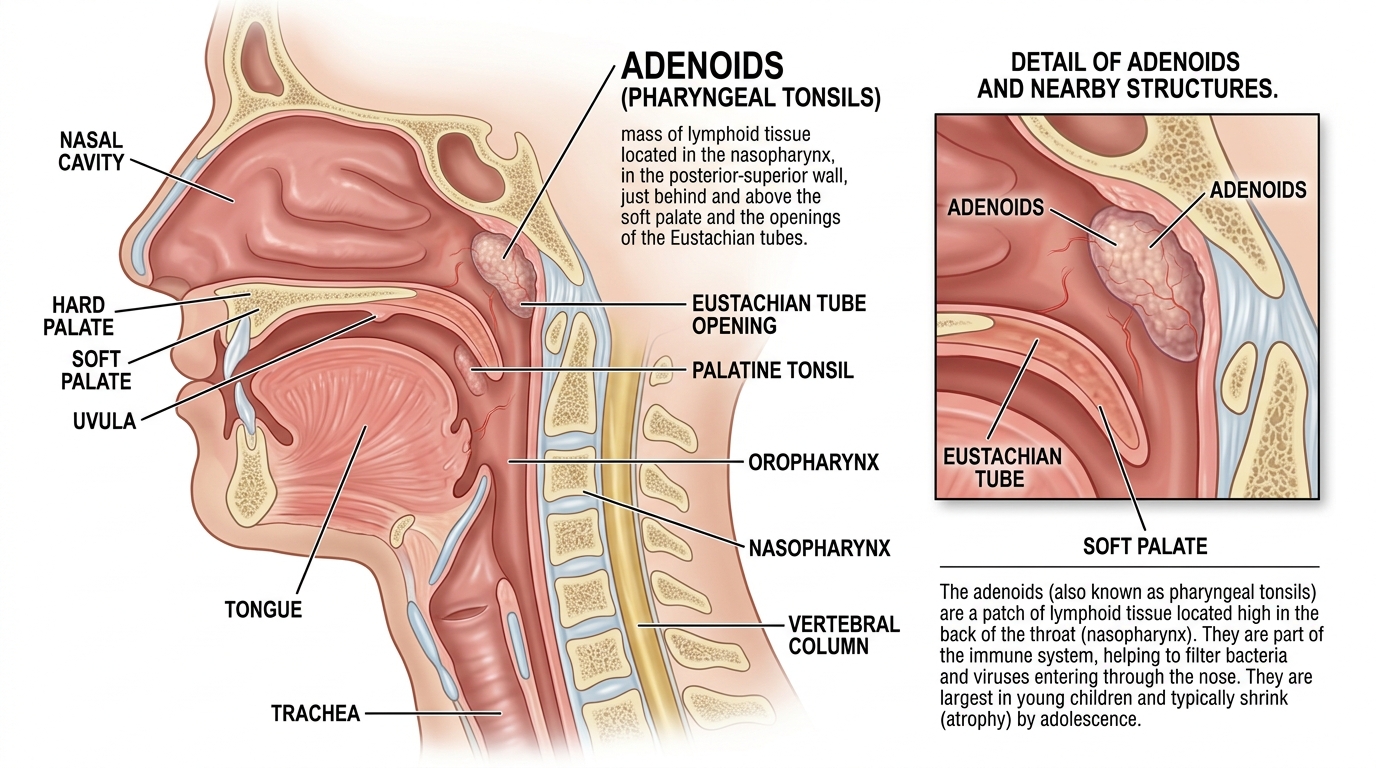
Before understanding this condition fully, you need a clear picture of what adenoids actually are and what they do. Specifically, adenoids are small masses of lymphatic tissue sitting at the junction where the nasal passages meet the back of the throat. Furthermore, they form part of the immune system’s first line of defense against bacteria and viruses entering through the nose.
In young children, adenoids work actively to sample and fight incoming pathogens before they spread further into the body. Additionally, they produce antibodies that help immature immune systems recognize and respond to infections more efficiently. Therefore, during early childhood, these glands serve a genuinely important protective function that supports overall immune development.
Interestingly, adenoids typically grow largest between the ages of three and seven before gradually shrinking through adolescence. Moreover, by adulthood, most people’s adenoids have almost completely disappeared without causing any problems whatsoever. Consequently, when problems do arise, they most commonly affect young children during the years when adenoids remain largest and most active.
However, when adenoids become chronically inflamed or persistently enlarged, they stop protecting the body and start obstructing it instead. Furthermore, this obstruction creates a cascade of symptoms that affect breathing, sleep, speech, and hearing in meaningful ways. Therefore, understanding when adenoids shift from helpful to harmful is central to recognizing this condition early.
Understanding What Adenoidid Actually Means
The term adenoidid specifically describes a state of chronic adenoid enlargement or inflammation that causes persistent clinical symptoms. Specifically, it goes beyond a single episode of swelling during a cold or flu and instead describes an ongoing problematic condition. Furthermore, this persistence distinguishes it from temporary adenoid swelling that resolves naturally after an acute infection clears.
Many parents encounter this term when their child develops recurring breathing difficulties, snoring, or chronic ear infections. Additionally, adults occasionally develop similar presentations when residual adenoid tissue becomes inflamed due to chronic allergies or infections. Therefore, this condition deserves attention across multiple age groups rather than being dismissed as exclusively a childhood concern.
Moreover, the clinical significance of this condition extends beyond simple discomfort. Untreated chronic obstruction can affect facial bone development in young children, alter sleep architecture, and impair academic performance. Consequently, early recognition and appropriate management prevent complications that become increasingly difficult to reverse over time.
Common Symptoms Patients and Caregivers Should Recognize
Recognizing the symptom profile of this condition helps families and clinicians move toward faster and more accurate identification. Specifically, persistent nasal obstruction that makes breathing through the nose difficult or impossible represents the most defining symptom. Furthermore, children with this condition often develop a characteristic open-mouthed appearance because nasal breathing simply becomes too effortful.
Snoring and noisy breathing during sleep frequently alarm parents and serve as early warning signs worth investigating promptly. Additionally, some children develop obstructive sleep apnea — a serious condition where breathing repeatedly stops during sleep — as a direct consequence. Therefore, any child who snores consistently or appears restless during sleep deserves a thorough ENT evaluation without delay.
A nasal quality to the voice, often described as hyponasal speech, develops when enlarged tissue blocks normal sound resonance through the nasal cavity. Moreover, this voice change is often the first sign that parents notice, prompting them to seek medical advice for their child. Consequently, speech changes in young children always merit clinical attention rather than casual dismissal.
Chronic runny nose with thick, discolored mucus also features prominently in many patients dealing with this condition. Specifically, the blocked nasal drainage creates an ideal environment for bacterial growth and persistent low-grade infection. Furthermore, this creates a frustrating cycle where infection worsens swelling, which in turn worsens drainage, which sustains further infection.
Recurrent ear infections and hearing difficulties affect a significant portion of children with this condition. Additionally, enlarged adenoid tissue sits directly adjacent to the openings of the Eustachian tubes, which regulate middle ear pressure and drainage. Therefore, when adenoid tissue blocks these openings, fluid accumulates in the middle ear, reducing hearing acuity and increasing infection risk.
Who Develops This Condition and Why
Understanding who develops this condition and what drives it helps families and clinicians make sense of an often confusing clinical picture. Specifically, young children between the ages of two and eight carry the highest risk because their adenoids are naturally largest during this developmental window. Furthermore, children who attend daycare or school encounter significantly higher pathogen loads that repeatedly challenge and stimulate adenoid tissue.
Allergies represent one of the most significant non-infectious drivers of chronic adenoid enlargement. Additionally, children and adults with allergic rhinitis experience persistent immune activation in their nasal passages that keeps adenoid tissue chronically inflamed. Consequently, addressing underlying allergies often produces meaningful improvement in adenoid-related symptoms without requiring surgical intervention.
Genetic predisposition also plays a meaningful role in who develops this condition. Specifically, children whose parents experienced adenoid problems in childhood face higher risk than the general population. Moreover, certain immune system variations appear to predispose individuals toward exaggerated lymphatic tissue responses to common environmental triggers.
Environmental factors like indoor air pollution, cigarette smoke exposure, and high allergen loads significantly worsen adenoid inflammation. Furthermore, children growing up in homes with smokers show markedly higher rates of adenoid and tonsil enlargement compared to children in smoke-free environments. Therefore, reducing environmental irritants forms a meaningful part of both prevention and management strategies.
Repeated upper respiratory infections, particularly bacterial infections of the nose and throat, create cumulative stimulation that keeps adenoid tissue persistently enlarged. Additionally, some bacteria form biofilms within adenoid tissue that resist standard antibiotic treatment and maintain chronic low-grade infection. Consequently, these biofilm-associated cases often prove the most resistant to conservative medical management.
How Clinicians Diagnose This Condition
Accurate diagnosis requires combining a thorough clinical history with appropriate physical examination and diagnostic tools. Specifically, the consultation typically begins with a detailed account of symptoms, their duration, severity, and impact on daily functioning. Furthermore, caregivers should bring notes documenting sleep patterns, breathing observations, and any related symptoms affecting ears or speech.
Physical examination by an ENT specialist provides the most direct assessment of adenoid size and condition. Additionally, clinicians use a small flexible camera called a nasopharyngoscope to directly visualize the adenoid tissue through the nasal passage. Therefore, this procedure gives clinicians precise information about the degree of obstruction and the tissue’s overall condition.
Lateral neck X-rays historically provided a simpler method for estimating adenoid size relative to the airway. Moreover, this remains a useful initial screening tool in settings where endoscopic equipment is unavailable or where patient cooperation is limited. Consequently, many community pediatricians still use X-rays as a first-line imaging approach before specialist referral.
Sleep studies, called polysomnography, help clinicians quantify the severity of sleep-disordered breathing in children with suspected sleep apnea. Specifically, these studies measure oxygen saturation, breathing pauses, heart rate, and sleep architecture throughout the night. Furthermore, the results guide treatment urgency and help families understand the full scope of their child’s nighttime difficulties.
Hearing tests help assess the degree of conductive hearing loss associated with middle ear fluid accumulation. Additionally, tympanometry measures middle ear pressure and helps identify fluid behind the eardrum in children who cannot reliably report hearing changes themselves. Therefore, audiological assessment forms an essential component of the complete diagnostic workup for this condition.
Conservative Treatment Options Worth Trying First
Many clinicians prefer starting with conservative management before considering surgical intervention, particularly in milder cases. Specifically, nasal saline irrigation helps clear mucus, reduce inflammation, and improve nasal airflow in children and adults with chronic nasal obstruction. Furthermore, regular irrigation is safe, inexpensive, and remarkably effective when patients and caregivers practice it consistently.
Intranasal corticosteroid sprays reduce adenoid tissue inflammation directly and consistently demonstrate benefit in clinical research. Additionally, these sprays work gradually over several weeks, so clinicians typically recommend a trial period of at least six to eight weeks before evaluating results. Therefore, patience and consistent application are both essential to giving this treatment a fair evaluation.
Antihistamines and allergy management medications help significantly when allergy-driven inflammation underlies the condition. Moreover, identifying and reducing exposure to specific allergens through environmental modifications can produce lasting improvements that medications alone cannot always achieve. Consequently, allergy testing and subsequent management represent a worthwhile investment for many affected patients.
Antibiotics treat acute bacterial infections that trigger flare-ups, but they offer limited benefit for chronic cases where biofilm formation has occurred. Furthermore, clinicians increasingly recognize that repeated antibiotic courses without addressing the underlying cause often provide diminishing returns over time. Therefore, antibiotic use requires thoughtful clinical judgment rather than reflexive prescribing in response to every symptom episode.
Surgical Treatment: Adenoidectomy
When conservative management fails to provide adequate relief, surgical removal of the adenoid tissue becomes the most appropriate next step. Specifically, an adenoidectomy is a relatively straightforward surgical procedure that ENT surgeons perform under general anesthesia in an outpatient setting. Furthermore, most children return home on the same day as their procedure and recover fully within one to two weeks.
The surgeon removes the adenoid tissue through the mouth using specialized instruments, without making any external incisions. Additionally, modern techniques use electrocautery or microdebriders that minimize bleeding and improve precision compared to older methods. Therefore, current adenoidectomy procedures carry low complication rates and deliver consistently favorable outcomes for appropriately selected patients.
Many surgeons recommend combining adenoidectomy with tonsillectomy when both tissue types show significant enlargement contributing to airway obstruction. Moreover, addressing both sources of obstruction simultaneously avoids the need for a second procedure and produces more comprehensive symptom relief. Consequently, combined surgery has become the standard approach for children with both adenoid and tonsil-related problems.
Insertion of ear tubes, called tympanostomy tubes, frequently accompanies adenoidectomy in children with recurrent ear infections or persistent middle ear fluid. Specifically, these tiny tubes restore Eustachian tube function by providing an alternative drainage pathway until the child’s anatomy matures. Furthermore, the combination of adenoidectomy and tube insertion dramatically reduces ear infection rates and improves hearing outcomes in affected children.
Recovery After Surgery and What Families Should Expect
Understanding the recovery process helps families prepare practically and emotionally for the period following surgical intervention. Specifically, most children experience mild to moderate throat pain, low-grade fever, and reduced appetite during the first several days after surgery. Furthermore, encouraging adequate fluid intake is the most critical priority during early recovery to prevent dehydration and support healing.
Soft foods like yogurt, ice cream, mashed potatoes, and soups keep nutrition adequate while minimizing discomfort during swallowing. Additionally, caregivers should avoid giving children hot, hard, or sharp-edged foods for at least one week following the procedure. Therefore, preparing a selection of appropriate foods before the surgery date reduces stress and confusion during the recovery period itself.
Most children return to school within one week, though complete tissue healing takes approximately two to three weeks. Moreover, strenuous physical activity warrants restriction during the initial recovery period to reduce bleeding risk. Consequently, families should plan school and activity schedules accordingly before the surgical date arrives.
Breathing improvements often become noticeable almost immediately after surgery, which many families describe as genuinely transformative. Additionally, sleep quality tends to improve dramatically within the first week, producing rapid positive changes in the child’s energy, mood, and behavior. Therefore, most families consider the recovery period well worthwhile given the magnitude of improvements that follow successful surgery.
Potential Complications and When to Call a Doctor
While adenoidectomy carries a low overall complication rate, families should recognize specific warning signs that require immediate medical attention. Specifically, bleeding from the mouth or nose beyond minor spotting warrants an immediate call to the surgical team or emergency department. Furthermore, high fever, inability to swallow liquids, or signs of respiratory distress also require prompt evaluation without hesitation.
Adenoid regrowth occurs in a small percentage of children, particularly those who undergo surgery at very young ages before their immune systems fully mature. Additionally, children with significant allergic disease carry higher regrowth risk because ongoing immune stimulation continues to drive lymphatic tissue proliferation. Consequently, managing underlying allergies after surgery remains important for maintaining long-term surgical results.
Long-Term Outlook for Patients With This Condition
The long-term outlook for children and adults who receive appropriate treatment for this condition is genuinely encouraging. Specifically, most children who undergo adenoidectomy experience permanent resolution of their nasal obstruction, sleep disturbances, and recurrent infections. Furthermore, improvements in hearing, speech, and sleep quality often produce secondary benefits in academic performance, behavior, and emotional regulation.
Children whose facial bone development was beginning to show the effects of chronic mouth breathing often demonstrate gradual normalization after successful treatment. Additionally, early intervention before significant facial changes become established produces the most complete resolution of these skeletal effects. Therefore, timely treatment decisions produce benefits extending well beyond simple symptom relief.
Adults with residual adenoid tissue causing symptoms also respond well to appropriate medical or surgical management. Moreover, addressing chronic nasal obstruction in adults improves sleep quality, reduces fatigue, and enhances overall quality of life in meaningful and measurable ways. Consequently, adults experiencing relevant symptoms should seek ENT evaluation rather than accepting chronic nasal obstruction as an inevitable adult problem.
Practical Tips for Parents and Caregivers
Navigating this condition as a caregiver requires practical knowledge alongside emotional patience and persistence. Specifically, keeping a symptom diary documenting snoring frequency, sleep quality, mouth breathing, and ear infection episodes helps clinicians make faster and more accurate decisions. Furthermore, photographs or short video recordings of nighttime breathing can provide invaluable clinical information that verbal descriptions alone rarely convey.
Maintaining smoke-free home environments, managing indoor allergens, and ensuring children receive recommended vaccinations all reduce the frequency and severity of upper respiratory infections. Additionally, breastfeeding during infancy supports immune system development in ways that may reduce adenoid-related problems later in childhood. Therefore, preventive health behaviors during early life carry genuine long-term benefits for children’s ENT health.
Final Thoughts
Adenoidid is a common but genuinely impactful condition that deserves prompt attention, accurate diagnosis, and thoughtful treatment planning from experienced clinicians. Furthermore, families who understand this condition clearly make better decisions, advocate more effectively, and support their children’s recovery with greater confidence and competence. Therefore, whether you are just beginning to investigate your child’s symptoms or already navigating treatment decisions, knowledge remains your most powerful and practical tool throughout this entire journey.